Uterine Fibroid Embolization Procedure
Uterine fibroids are common, benign, smooth muscle tumors involving the uterus that can become symptomatic in premenopausal women, resulting in abnormal bleeding, pain, and bulk among other symptoms. Uterine fibroid embolization (UFE) also known as uterine artery embolization (UAE) is a relatively new minimally invasive, non-surgical therapy option for women who wish to avoid surgery or long-term medical therapy. It works on the basis of eliminating the blood flow to the fibroids, resulting in their shrinkage and controlling their symptoms while preserving the uterus.
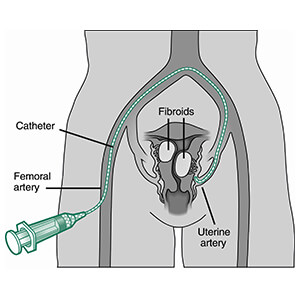 The procedure of uterine artery embolization was introduced in 1995 and involves placing a catheter in the groin in the common femoral artery. This is done in a hospital setting in an interventional radiology suite or lab, using sterile technique and utilizing both conscious sedation and local anesthesia.
The procedure of uterine artery embolization was introduced in 1995 and involves placing a catheter in the groin in the common femoral artery. This is done in a hospital setting in an interventional radiology suite or lab, using sterile technique and utilizing both conscious sedation and local anesthesia.
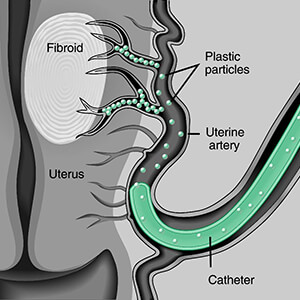
A diagnostic arteriogram or study of the blood vessels of the pelvis is then obtained and the two arteries supplying the uterus are identified. Using a smaller catheter and fluoroscopic guidance, one uterine artery is catheterized and once satisfactory position of the catheter is confirmed with xray imaging, the uterine artery is blocked or embolized with small rounded particles which collect in largest numbers in the benign growths known as fibroids, depriving them of their blood supply and causing them to shrink.
 Next, the tube or catheter is moved to the opposite side of the pelvis and the other uterine artery is treated in a similar fashion. The catheter is then removed and pressure is applied to the groin vessels to stop them from bleeding.
Next, the tube or catheter is moved to the opposite side of the pelvis and the other uterine artery is treated in a similar fashion. The catheter is then removed and pressure is applied to the groin vessels to stop them from bleeding.
The patient is then transferred to a recovery room and subsequently to a hospital room for observation and treatment of any pain that might ensue. Pain control is achieved with intravenous and oral medications, and a patient-contolled analgesia pump.
Considerations
Prior to undergoing the procedure, the patient is evaluated in a clinic setting by an interventional radiologist, who has undergone special training in catheter–based treatments. He or she will obtain an MRI (magnetic resonance imaging) which is a standard exam obtained without radiation, which helps to quantify the number of fibroids, their size, blood flow and location, all of which might determine how and if therapy will be beneficial. In addition, MRI has the benefit of evaluating for other conditions or tumors which might be present, such as adenomyosis or tumors of the ovary.
Should fibroids be present which have a pedicle or stalk that projects into the pelvis or uterine cavity, it might not be safe to undergoe UAE. In addition, the radiologist will conduct a history and physical and review the patient’s medications and other conditions to see if the patient is a candidate for the procedure. The evaluation will include a discussion of the alternatives available to the patient. Laboratory tests will be ordered and additional test such as a PAP smear and endometrial biopsy will be discussed prior to the procedure.
After the procedure, the patient will experience some pain, ranging from mild to severe, which is usually well controlled with medications. The patient will generally be discharged to home the following morning with a follow-up clinic appointment in 2 to 6 months. The patient will be sent home on oral pain, antiflammatory and antinausea medications and will be checked on by nursing staff by phone the next day. The patient may experience the following:
- discharge
- post embolization syndrome (pelvic pain, cramping, low grade fever, muscle aches and pains, malaise, fatigue)
- premature menopause
- fever
- infection
These will be discussed with your physician prior to the procedure and will be closely monitored following the procedure. Complications are rare and may include need for a hysterectomy.The overall complication rate is very low measuring several percent.
Success Rates
The success rate of completing the procedure is very high, approaching 100%. Compared to hysterectomy, UAE took less time, had less blood loss, shorter hospital stay, and faster resumption to normal activities of daily living. Both groups hysterectomy and UAE patients were satisfied with their treatment. Short term, 85-94% of UAE patients see improvement in their bleeding. The uterus decreases in size by about half of its orginal volume. Bulk related symptoms improve in 60-94% of women. The Society of Interventional Radiology reports that 94% of women had significant improvements in their quality of life, but 14% had another invasive procedure (hysterectomy 9.8%, myomectomy 2.8%, repeat UFE 1.2%) to help with their symptoms.
Long term, the success rate of UAE approaches 75% with women reporting normal or improved symptoms. Only about 20% of the time will a UAE patient need a second procedure due to persistent symptoms. Repeat UAE is often successful in controlling symptoms. The procedure is not generally utilized for those women desiring future fertility but there are reports of patients with successful pregnancies after UAE.
In summary, UAE is successful in controlling the symptoms of premenopausal women with symptomatic fibroids, has a high success rate, low complication rate, is a minimally invasive alternative to surgery, is associated with a short hospital stay and has a high satisfaction among women who undergo the procedure.
Uterine Fibroid Embolization Options in Colorado Springs, CO
Just like with all our radiologic imaging procedures, RIC Radiology is at the forefront of medical innovation, as interventional radiology continually advances in patient diagnosis, treatment and recovery. Minimally invasive treatment and therapy offer an alternative to conventional surgery by using less invasive techniques, especially endoscopes and vascular catheters. With less need for hospitalization, less post-operative morbidity, and early return to normal activities, minimally invasive procedures may gradually replace most present open surgeries.
Our radiologists are board certified and have attained Certification of Additional Qualification in Interventional Radiology and are the area’s experts in uterine fibroid embolization. Call today to schedule a consultation 719-471-3146.
Information and illustrations reprinted with permission of the Society of Interventional Radiology. For more information from SIR, visit their website: http://www.sirweb.org/patients/uterine-fibroids/